How we accomplished culture change virtually overnight — and why we wouldn’t necessarily recommend it as a strategy
Greetings from Atlanta!
The story I’m going to tell this month is truly unique in my decades of leading physician services programs. It starts when we won the contract to take over a system-wide hospitalist program that sees 180,000 patients per year spread over seven facilities.
We knew we had a big lift ahead of us in terms of recruiting. We needed to hire nearly 100 clinicians to staff the program. What we didn’t know is just how many barriers had been erected by the outgoing group for us to do that.
In the end, Core was able to recruit all the clinicians we needed AND transform the culture of the program for the better virtually overnight—but the story of how we got there isn’t exactly a model I’d recommend following.
It is, however, a story worth sharing because it highlights how good decisions and preparation, an experienced team, and a little luck can go a long way toward avoiding what otherwise could have turned out to be an expensive disaster:
Part 1: We Have a Problem
It was August 2021 when Core learned we had been selected to take over the program. The RFP had gone out to 14 national groups, 10 submitted proposals, and 4 companies came on-site to present in person. When Core was selected, it was a huge validation for our model.
But we knew the task ahead was large. The contract start date was March 1, 2022—six months away. Before then, we’d need to hire nearly 100 clinicians, along with a system medical director.
There was only one problem: each of the current hospitalists had a non-compete, and the health system had a non-solicitation agreement in place with the outgoing group. This meant there could be no help whatsoever in recruiting the existing physicians. No soft introductions, no phone numbers or email addresses—not even a list of who was there.
A little about non-solicitation clauses for physicians
Non-solicits for physicians are fairly common, especially in smaller, rural hospitals. In those cases, a huge part of the job of any physician services group is to do the work of recruiting physicians into the community. In those cases, a non-solicit clause protects the group from having the hospital take over the contract as soon as the job of recruiting is done.
In this case, however, there were two differences. First, it was a large system in a sizeable metro area. In that case, the job of a physician services company should be much more than simply being a staffing company. We consider our role to partner with health systems on every operational priority they have, starting with improving quality and reducing inpatient length of stay.
My feeling, especially at big, urban systems, is that we should continue to serve the hospital on the strength of our operational excellence and commitment to patient care. If one day the hospital should decide that we are falling short on those commitments, the physicians we recruited into that community are ultimately members of that community and should decide for themselves whether to stay or leave.
The second difference about this particular non-compete clause is that, unlike standard agreements, this one had no amount of money that could be offered as compensation to buy the physicians out of the agreement. In short, this felt like an unusually ironclad agreement, not intended to fairly compensate an outgoing group, but rather more intended to raise the threat of lawsuits.
Adventures in hospitalist recruiting
I’ve led a lot of programs in my career, and overseen a lot of transitions from one physician group to another—but I’d never been in the position of not even having a list of the existing physicians. Our retention rate for hiring existing clinicians is close to 100%. At every site we go into, if a hospital wants us to keep a clinician, we keep them.
So I figured we’d figure it out, and meanwhile, we immediately started building infrastructure locally. Our plan was to hire a local system director and either an MBA or MHA healthcare executive to oversee operations.
To kickstart the recruiting work, together with Wins Mathew, Core’s VP of Operations, we went onsite in Tulsa. We had no names or contact information for any of the hospitalists, just access to the conference room across from the doctor’s lounge. We met with administrators and we met with specialists. But meeting the hospitalists was another matter.
That first day, we were literally walking into the lounge, introducing ourselves to clinicians, and asking them if they were a hospitalist. The response we got was… cold. The doctors would talk to us for about thirty seconds, and then excuse themselves and say they had to go. It felt like something was off. It felt like they were scared to talk to us.
Eventually, someone told us what was going on. The owner of the outgoing group had told everyone not to talk to us, and that if they did, they wouldn’t have a job. This doctor had told them the transition wouldn’t work, that we wouldn’t be able to hire anyone, and that the health system would eventually ask him and his group to stay on.
The second time around, Wins went back to the hospital and posted flyers saying the time and place when we would be back, and inviting anyone to come chat. Again, no one came.
We decided to rent out a room at a local restaurant. Again, we advertised inside the hospital: food, drinks, and an offsite location to talk about the transition. The day before the event, our source told us that no one would be coming, because they were told if they did, they wouldn’t have a job. Two people showed up.
Part 2: When preparation meets opportunity
There’s a good saying: luck is when preparation meets opportunity.
We had a huge task ahead of us in recruiting dozens of physicians and nurses to work in our new program, but in the meantime, we also got to hiring a local system director. Before long we found the perfect candidate: the person we hired had worked in the city their whole career, had gone to residency there, and knew many of the local physicians.
Along with the system medical director, we hired a local director of operations and a local dedicated physician recruiter. Both of these hires were part of our commitment to having “boots on the ground” to ensure the partnership was successful.
Connecting with the existing hospitalists was still a major challenge, but in the meantime, we were getting major interest from doctors outside of town, and from residents. Still, we were a long way away from hiring everyone we needed. It looked like we might have to rely on locums agencies or other temproary help until we could get the residents there in July.
Then, our preparation met a great opportunity.
Who do physicians want to work for?
In December, the other major health system in town selected a big, national group to take over its hospitalist program. Pretty soon, it became clear that this group was doing a poor job of introducing itself to the existing physicians.
These doctors didn’t want to work for the national group. So we made a pitch: the opportunity to build a new program from the ground up. A reasonable work-life balance. A compensation package that had a competitive base salary, plus a productivity component that gave extra if it was busier than we intended to be.
Plus, Core Clinical Partners is a physician-owned, physician-led, physician-founded company with room to grow and control over our future. Our decisions are not influenced by a private equity firm or any other outside decision-makers. Our fate is our own.
It was a good pitch, and we were able to hire 35 doctors and APPs from the other health system.
Part 3: Culture Change Overnight
By January, things were coming together for the March 1 start date. Rather than rely on locums, we had been able to hire physicians from in town, from out of town, and out of residency.
We had less than two months to get many of them onboarded into the Core system. Interestingly, many of them had never used Epic before, so we did trainings on the system. We toured people around the hospital, we got them credentialed, and our team basically moved heaven and earth to get everyone ready.
In the end, only 12 clinicians were retained from the old group. We added 74 clinicians locally that we recruited and onboarded, and another 12 from out of the area.
To be clear: I would not recommend this strategy to anyone. Many of the existing physicians who had served the community for a long time ended up moving out of town. But there was a silver lining to launching a large hospitalist program with essentially a whole new team: we could do things our way from the start.
Normally, when we take on a new program, I am careful in what I promise to hospital administrators. I know we can decrease length of stay, and make meaningful improvements on quality and patient satisfaction, but I also know those changes take time.
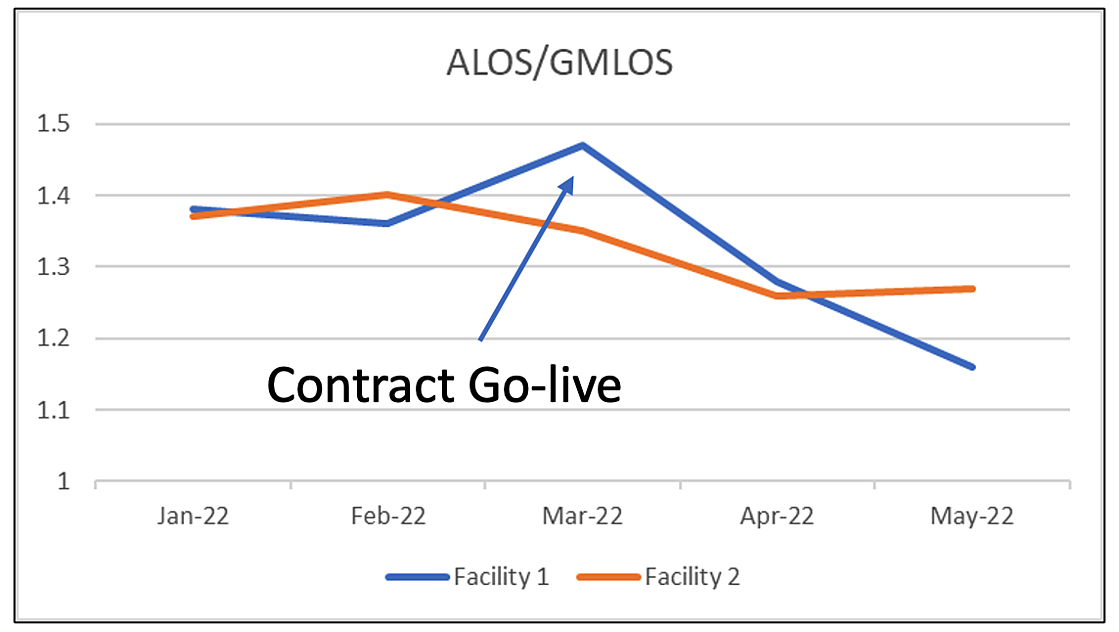
This time, these changes happened virtually overnight. In the first month at the largest hospital in the system, we decreased actual length of stay by almost a full day, resulting in a 20% drop in Geometric Index. That is simply unheard of. Here’s the ALOS/GMLOS chart from that first month:
Some other changes we were able to make right away. For instance, with the previous group mornings had often been a little chaotic. Their morning assignment of patients was not always done by 7 am, so physicians would sometimes come in and not know who they were supposed to see.
We fixed this overnight so every doctor who came in had a list of who their patients were, and where they were. We implemented a geographic rounding program that was in place on Day 1. We were able to fix night cross-coverage so patients who got seen at night also got admitted at night, whereas in the previous group these patients often had to wait much longer. Our doctors were much more available to nurses and case management, so we were able to get decisions made more quickly and efficiently.
Our system-level director of operations oversaw everything and pulled it all together, from schedules to staffing shifts, and chart flow—all of the things you need to make the operation successful.
Finally, the team we brought in was simply a great team. I am very proud of the work our recruiters did to hire so many people so fast, and I want to extend my thanks and appreciation to all the excellent clinicians who are working in the hospitalist program today, and who signed with us earlier during the transition. They took a chance with a new group and a new system, and as a result, they are making a difference for the patients, for the hospital, and for the community.